



From the previous part, we learned that nothing takes as many lives as high blood pressure (BP). We also found out that strength athletes are ahead of both other athletes and ordinary people both in the high blood pressure chart.
There is a reason for it: Not every training causes growth – only the one that gives a correct amount of stress that promotes an adaptation – growth, strength gain, etc.
When you get stressed out your body switches from the restful nervous system state called the parasympathetic nervous system to the sympathetic nervous system state which is a more vigilant state.
When you're in the sympathetic nervous system state your blood vessels constrict and your heart rate rises to make you the most physically capable.
But in the long term perspective this causes undue strain on the heart where the heart has to pump blood through your blood vessels if they're constricted your heart has to pump harder, in a result, it grows.
As the heart grows it develops pathological behavior and particularly high blood pressure.
The body organs and systems of a weightlifter athlete undergo various morphological and functional changes as the loads increase and the degree of adaptation to them increases. In the process of training, functional adaptive changes also develop in the work of the cardiovascular system, which are supported by morphological restructuring ("structural trace") of the circulatory system and some internal organs.
This adaptive restructuring provides the cardiovascular system with high performance, allowing the athlete to endure intense and prolonged physical activity. But every coin has two sides, and systematic high blood pressure is one of the side effects of this adaptive restructuring.
This applies even more to bodybuilding than to classic weightlifting. Despite the fact that professional bodybuilders take better care of their health than ordinary people, however, as experience shows, they live less and die more often.
Let's remember the most famous cases:
Cedric McMillan died of a heart attack at the age of 44 , Shawn Rhoden 46 died of a heart attack, Paul Poloczek 37, Alena Kosinova 49, Sofia Graham 27, Orlando Gallucci 33, Tom Prince 52 , Dave Draper 79 heart failure,
Bostin Loyd Dies At 29 Years Old of cardiac arrest, George Peterson 37 heart attack, Shawn Rhoden, who became the oldest person to win the prestigious Mr. Olympia title at the age of 43 in 2018, suffered a fatal heart attack in November. Female bodybuilder Odalis Santos Mena, 23, suffered cardiac arrest and died following a botched operation to stop her excess underarm sweat, Mr. England runner-up Ben Harnett, 37, died in 2019 after taking steroids before a bodybuilding event.
And famous Zyzz suffered a heart attack and died at the age of 22!
This list can be much longer…
An impressive piece of work has been done by thebarbell.com [1]. They summed up the statistics on the deaths of 60 pro bodybuilders:
- 25 Cardiovascular (17 heart attacks, 6 heart failures, 1 vasculitis, 1 aneurism)
- 11 Unspecified Natural Cause (includes 5 unreleased cause)
- 7 Cancer (2 stomach, 2 leukemia, 2 unspecified, 1 skin)
- 6 Kidney (3 kidney failures, 1 multiple organ failure, 1 failed kidney transplant, 1 sudden decline/chronic kidney disease)
- 6 Unnatural (2 murders, 2 suicides, 1 overdose, 1 accidental)
- 2 Brain (2 Alzheimer’s disease)
- 2 Lung (1 Valley Fever, 1 pneumonia)
- 1 Liver (1 liver failure)
Cardiovascular issues cause more than 40% of deaths! This is more than the general population of people, and more than weightlifters in a previous part of this article!
Now let’s chart those causes as well as the causes for all American men. The average year of death for our 60 pro bodybuilders was 2008, so we used statistics for male deaths for that year from the Center for Disease Control’s National Vital Statistics report.[1] [2]
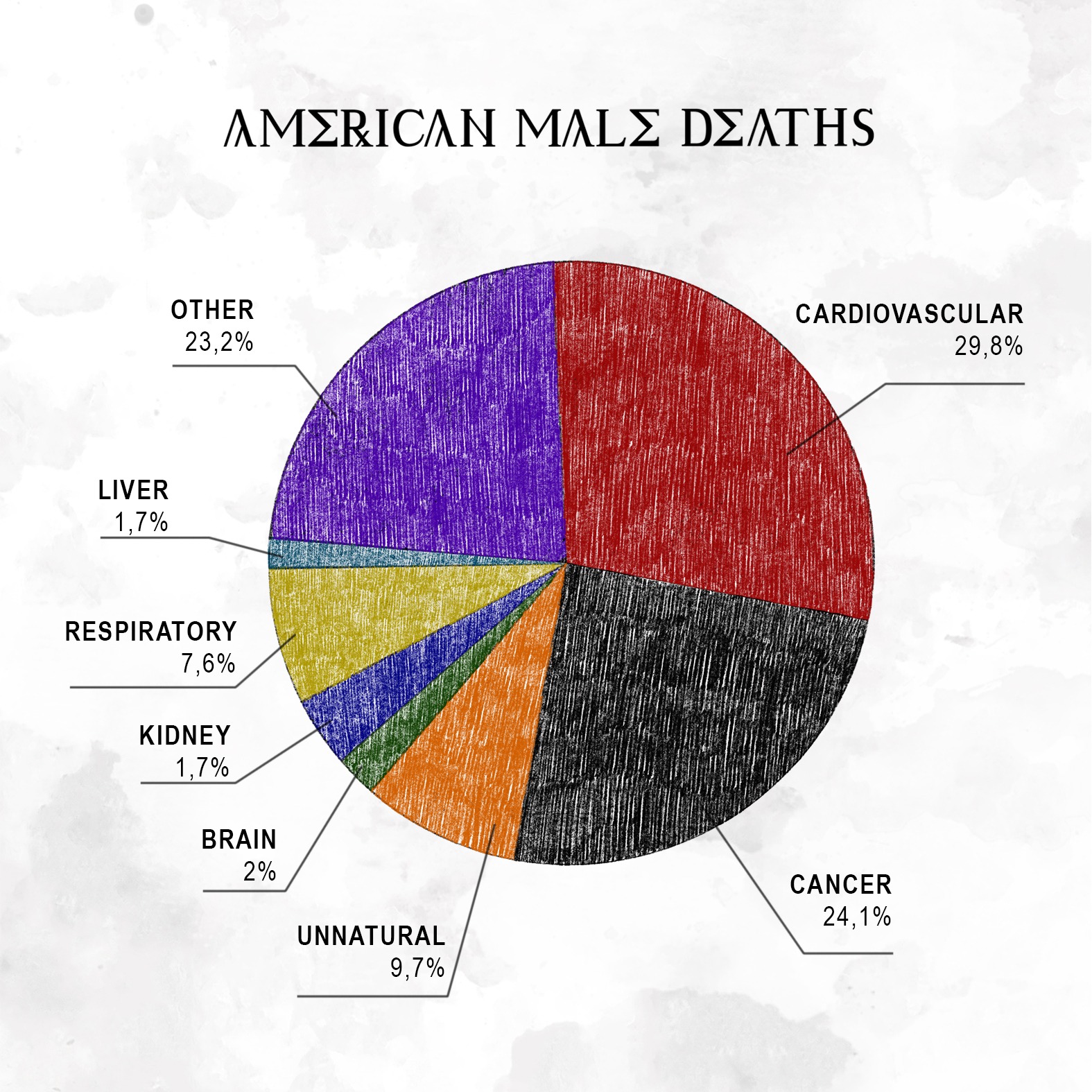
Of the 60 pro bodybuilder deaths, 25 are known to be heart-related (and likely more from the “unspecified natural” category). Shockingly, 10 of these occurred in bodybuilders under 45 (out of 18 deaths), 55.6%. Such deaths should be very rare. Conversely, only 2 of the 12 deaths of pro bodybuilders over 65 were cardiovascular (16.6%), about half the rate of all 65+ American men. When we chart by age groups—young adult (20-44), middle-aged (45-64), and senior (65+)—to show what percentage of deaths in each group were cardiovascular, it’s shocking to see pro bodybuilder deaths descend from sky-high to very-high to low while American male deaths ascend from very-low to high and to very-high.

Heart disease is the leading cause of death in America and worldwide. Still, the 25 pro bodybuilder cardiovascular deaths stand out. If six or more of the 11 deaths listed as “unspecified natural” were heart-related, over half of the pro bodybuilder deaths have been cardiovascular. This is alarming, but even more so when we consider the young age at which too many pro bodybuilders are dying from heart failure.
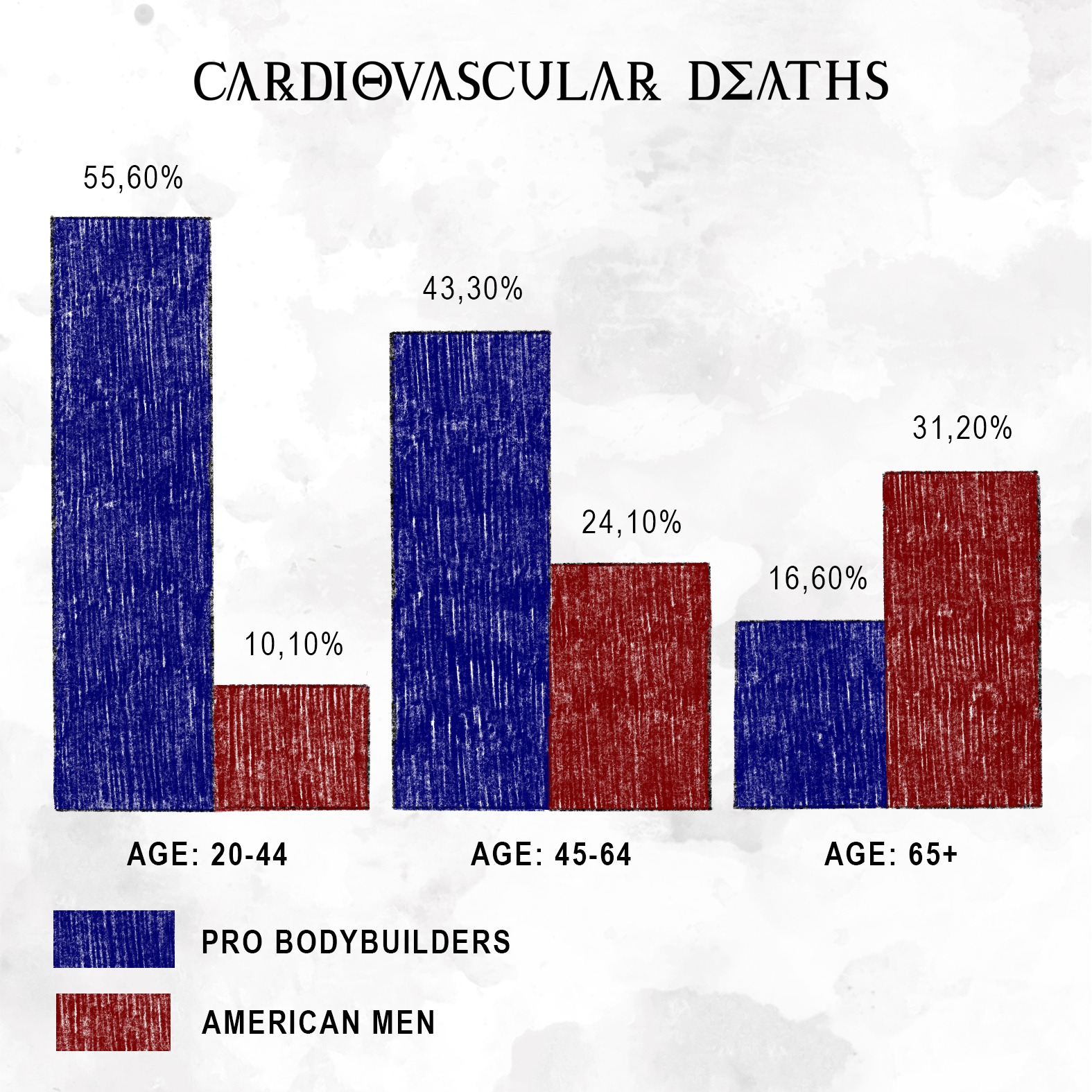
The first two blue bars are very alarming, especially when you consider that the greatest factors for heart disease (obesity, diabetes, smoking, lack of exercise) are largely disassociated from bodybuilding. Furthermore, a 2018 study demonstrated weight-training may greatly reduce the risks of heart attack and stroke.[2]
Ideally, all the blue bars should be half as high as their red counterparts. Young or middle-aged men with low bodyfat who regularly exercise should not be dying of cardiovascular maladies at the same rate—let alone a much greater rate—as men of all ages. The most likely culprit is performance-enhancing drugs. [1]
And this is despite the fact that we are not talking about amateurs whose health care is not a part of the professional routine, so sometimes they save on it, we are talking about professional athletes who employ a whole staff of proven specialists.
Based on this reflection, it becomes clear that among amateurs, the results are expected to be even worse.
So cardiovascular disease is the top cause of death globally. High blood pressure is a No 1 risk factor and guys who are lifting weights suffer more from it. Bodybuilders as a special case of weightlifters are identified as the highest risk group according to statistics.
Standard recommendations for bodybuilders who have been given by doctors since the mid-60s: to restrict sodium intake, control weight, and use relaxation techniques – are base recommendations to reduce the high BP, are useful, but definitely not enough.
One of the significant risk factors is performance-enhancing drugs(PEDs) and in particular steroids.
Anabolic steroids that make it possible to achieve superhuman strength and volume have a noticeable effect on increasing the risk of cardiovascular issues.
Usually, people pay little attention to the side effects of such drugs: everyone is more interested in the anabolic and androgenic index, the likelihood of baldness or aromatization, but important factors
This mechanism of increase of blood pressure by anabolic steroids has been well studied.
Anabolic steroids are able to increase the reactivity of the vascular wall to norepinephrine, increase plasma renin activity, stimulate the production of aldosterone and increase sodium retention by the kidneys. As a rule, this problem is dose-dependent (dose = effect). Steroids also increase hematocrit and circulating blood volume.
The effect of steroids on blood pressure can persist for a long time; some studies have shown a persistent increase up to 12 months after stopping steroids.
To a greater extent, the problem of hypertension is associated with taking drugs with increased conversion to estrogen or having an estrogenic effect.
The fact is that drugs, that make you strong directly raise the blood pressure most, like trenbolone and oxymetholone it affects your sympathetic nervous system and increases the dopamine/noradrenaline/adrenaline release, which spikes your BP really high.
So, at the moment, pressure problems are the most common in bodybuilding/powerlifting community. This problem will be completely solved only in the future, but at the moment there are several groups of drugs to reduce pressure.
The first line of treatment and prevention of high blood pressure in modern medicine is a class of medications called angiotensin II receptor blockers(ARB).
ARBs block the action of a hormone called Angiotensin II, which is produced naturally by our bodies, causes our blood vessels to constrict and tells our kidneys to retain water, and too much of this hormone may lead to high blood pressure over time. Medications like losartan block the hormone from acting in our bodies in order to lower blood pressure
Just a very quick summary… most popular ARBs are :
Valsartan is the most selective it's like the surgical approach but again not the strongest at the higher doses.
Irbesartan has some unusual properties. Studies showed that it may be helpful in chronic kidney disease.
Azilsartan is the most powerful at the max dosage
Telmisartan is the one, that has the least number of negative side effects. But dozens of positive side effects.
Let’s talk about Telmisartans undeniable benefits more:
It lowers your pressure and at the same time it is a PPAR-γ receptor gamma agonist which means it helps you put fat in adipocytes instead of your blood and visceral fat.
Telmisartan proved to be effective not only in controlling blood pressure, but had a favorable effect on lipid profile also. [3]
As you know, a poor lipid profile worsens the condition of blood vessels, which can serve as an additional cause of increased pressure, as well as an additional risk of mortality due to the formation of plaques and blood clots in the vessels. The use of anabolic steroids greatly spoils the lipid profile and it’s a big issue.
Anabolic steroids cause marked high-density lipoprotein level depression (weighted average, 52%) and severe depression of high-density lipoprotein-b levels (weighted average, 78%) while raising low-density lipoprotein levels an average of 36%.[4]
And again: this mechanism reduces visceral fat that is guilty of metabolic disturbances and increased risk for cardiovascular disease and type 2 diabetes.[5]
And it makes sense cos Telmisartan has shown a positive effect in the treatment of insulin resistance, diabetes, and metabolic syndrome, whose activation is also correlated to anti-inflammatory and finally, anti-atherosclerotic properties.
Another important issue is left ventricular hypertrophy - a thickening of the wall of the heart's main pumping chamber. The second and more popular name of this syndrome will tell you everything about its nature - The Athlete's Heart. It’s a direct aftermath of lifting weights “Resistance training induces the development of concentric cardiac hypertrophy”©[6]
This is a very extensive topic, and it deserves a separate article, but it should be noted that Telmisartan has studied positive effects here too, and has already been used in clinical practice in this case.[7]
In terms of the number of positive effects and the small number of negative side effects for the athlete, this drug is an absolute champion, so we included it in our assortment.
We find this ARB the best for all weightlifters, bodybuilders and especially steroid users.
It has 24 hours half-life so can be taken once a day, so you have more time for cooking, napping, pumping the iron, and making injections.
Telmisartan has the greatest bioavailability - 43% of all ARBs witch for example almost twice bigger as valsartan - 23%.
And the cherry on the cake of all ARB class medication and Telmisartan, in particular, which is extremely profitable for the athletes. As the latest studies have shown that improve Angiotension receptor blockade administrated muscle regeneration [8].
That’s- the thing you need to recover after hardcore training better!
The properties of lowering hematocrit have also been proven [5], but it only manifests itself in those who have a high hematocrit [6]. Among the users of PED and boldenone in particular, these are the majority, I'm sure.
Another cool feature for all ARBs is “Angiogenesis”. This term means the development of new vascular structures in your body and all ARB improves angiogenesis, which may explain the accelerated recovery of skeletal muscle injuries while taking sartans, but there is also a negative side (it is always there, damn it!).
Angiogenesis can lead to accelerated growth of tumors and during the studies some increases have been seen in other ARBs but not in Telmisartan. It has NO effect on tumor growth. Its study proved and that's great news! [11]
“Compared with other ARBs, telmisartan is not associated with an increased risk of cancer. This study provides reassurance as to the short-term safety of telmisartan.” © [11]
In clinical practice, Telmisartan is used alone or together with other medicines to treat high blood pressure (hypertension). High blood pressure adds to the workload of the heart and arteries. If it continues for a long time, the heart and arteries may not function properly. This can damage the blood vessels of the brain, heart, and kidneys, resulting in a stroke, heart failure, or kidney failure. Lowering blood pressure can reduce the risk of strokes and heart attacks.
Previously, high mortality due to heart and kidney problems was a serious threat to all those who do sports and cross the 30-year mark. Blood pressure generally tends to increase with age:
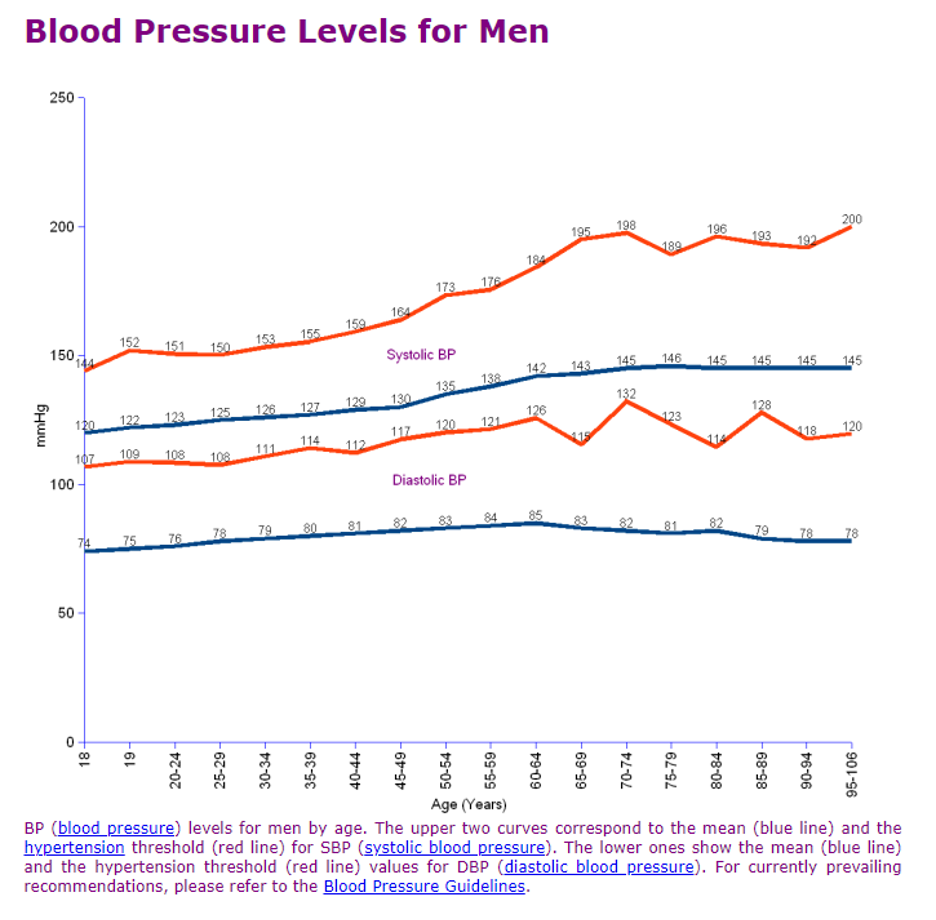
This means that the older we are, the more predisposed to the mortal danger of high blood pressure.
Our advice:
Get an annual physical with bloodwork (raise the frequency if you use steroids, and i know, you do) and monitor your own blood pressure regularly (you can buy a cheapest monitor for under 20e) to make certain it stays in the normal range. Furthermore, do not ignore warning signs like elevated cholesterol or high blood pressure, but take appropriate steps to reduce these to safe ranges, even if this means halting a drug cycle or ending a contest prep.
Too many people die from this every day.
We recommend you pay attention to blood pressure and use Telmisartan at the first sign of its increase, whether due to steroids and training, or for age reasons.
High blood pressure kills.
Yes, this drug will have a minor positive effect on your muscle growth, but it will be very useful in prolonging your healthy and fulfilling life.
As the example of Zyss showed, it is possible to die from the side effects of steroids even at 22.
Now, when you know how important and beneficial this drug is, and you are a bodybuilder and you taking steroids..... is there an excuse to not take telmisartan?
When people say it's not healthy to take steroids, I say it's not healthy to take them without telmisartan (c) Tony Huge
P.S. We will make a small addition to this article in which we will give a brief overview of other pressure control tools that may well work in certain cases, but telmisartan is available in Driada shop already!
Stay healthy, gentlemen!
[1] https://www.thebarbell.com/do-pro-bodybuilders-die-younger-than-average
[2] https://www.cdc.gov/nchs/data/nvsr/nvsr60/nvsr60_06.pdf
[4] https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/615569
[5] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4800358
[6] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1905938
[7] https://academic.oup.com/ajh/article/27/2/260/2743098
[8] https://pubmed.ncbi.nlm.nih.gov/18550776
[9] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3416676
[10] https://www.ejinme.com/article/S0953-6205(15)00442-2/fulltext
Leave a Comment