



In this article, we will introduce you to several concepts for your first cycle and describe each of them.
General rules
The first cycle must necessarily be based on one steroid drug or two, including testosterone. The use of cycles consisting of two drugs makes sense until they can significantly affect the athlete's body, since their effect will gradually decrease, and at some point the athlete will have to switch to complex cycles of steroid drugs (or significantly raise the dosage).
You can use complex cycles of steroid drugs when simple cycles no longer meet all the needs of an athlete. It is worth first switching to a cycle of three drugs, eventually increasing the number of compounds in each cycle.
The main task for the first cycle, in my opinion, is to monitor the response of your body. The choice of drugs in this case will not depend on your intended goals (gaining muscle mass, losing fat, increasing endurance), since this first cycle is considered as an attempt to understand your reaction to taking anabolic steroids. After completing the first cycle, you will be able to evaluate the result, and then make more complex cycles, setting certain goals.
Duration
It is not recommended to do the first cycle lasting more than 10 weeks. During this time you can already get some visible results and at the same time get a minimum of long term side effects. Also, after a 6-10 weeks cycle, you can quickly restore your own testosterone levels and thereby maintain the result. Usually, If you have been training for a long time already and are doing everything correctly, then the first cycle is going to be very effective, and most of the muscle mass will remain with you forever.
For your first cycle, you should select the mildest drugs. This is already much more than your natural hormonal background, so If you can make progress on soft drugs and minimal dosages, consider yourself very lucky and you can repeat this regimen repeatedly until it stops working for you.
Popular PEDs for the first cycle
Below is a list of the most popular steroids and SARMs that you can use during your first cycle along with testosterone.
Anavaros (Oxandrolone)
Has an extremely low level of androgenic activity with a high anabolic index. The drug is great for beginners because it has a minimal side effect. Recommended dosage is 20-40 mg/day.
Turinadyn (Turinabol)
Significantly increases muscle growth and strength. It is valued for its good tolerance and low amount of side effects. Recommended dosage is 20-40 mg/day.
Primos (Methenolone, oral or injectable)

These drugs are also considered as the mildest in terms of their effect, so they are quite suitable for the first cycle. The recommended dosage is 50 mg/day for the oral form and 200 mg per week for the injectable form.
Ostarine
The most selective and therefore the safest SARM in terms of side effects. Increases lean muscle mass and strength, but is superior to other SARMs when it comes to safety.
If you use this SARM in minimal dosages, the suppression of endogenous testosterone is likely to be minimal, which is the great thing for your first cycle.
Testolone (RAD140)
Effectively increases muscle mass, strength and gives a ripped look and pronounced venousness. Athletes experience greater fullness and stiffness during the intake.
If you use this SARM in minimal dosages, the suppression of endogenous testosterone is likely to be minimal, which is great for your first cycle.
Andarin (S4)
Significantly increases muscle mass, strength performance and burns fat, which together gives athletes a ripped look and venousness.
If you use this SARM in minimal dosages, the suppression of endogenous testosterone is likely to be minimal, which is great for your first cycle.
Fear of injections
Usually, beginners do not want to do intramuscular injections, they want to do their first cycle using only oral medications. This can be easily understood - because for them, the use of anabolic steroids seems to be something new, unexplored and even frightening, especially taking into account the many popular myths about steroids inspired by the media. On the other hand, the idea that oral steroids are safer is a mistake, because injectable drugs have much less effect on the liver.
The only factor in favor of oral medications is their short half-life, which, if something goes wrong, will make it possible to quickly cancel the drug. But "something will go wrong" is an extremely rare case. Usually, the side effects of anabolic steroids are not so dangerous that their rapid refusal to take them would be of significant importance.
We also have another problem - the lack of an effective and safe form of oral testosterone.There are two forms of oral testosterone in total - methyltestosterone, which is extremely toxic and should not be used, and oral testosterone undecanoate (capsules), which have low bioactivity, therefore its intake does not give the desired effect.
Read here why testosterone should always be in your cycle.
We must remember a simple thing - the only form of testosterone that is available to us is injectable testosterone. It is for this reason that your first cycle should in any case consist not only of oral steroids but also of testosterone injections. Next, we will also talk about several options when intramuscular injections can be avoided and replaced with subcutaneous ones.
What to do if I don’t want to do intermuscular oil injections
There is a number of people who do not use testosterone because they are afraid of intramuscular injections. Unfortunately, there are only two types of oral testosterone: testosterone undecanoate, which is very rare on the market, and methyltestosterone, which is toxic enough to take for a long time. In this case, there are two alternative options and both of them involve the use of subcutaneous injections.
Subcutaneous injections of testosterone
When using this option, you simply change the intramuscular injection needles to small 12 mm long insulin needles with which you will inject testosterone under the skin. Such injections are painless. We should immediately warn that this method is not used in official medicine, but there are many people who do just that.
The peculiarity of these injections is that you cannot use large amounts of oil at one time, you will have to divide your dosage into many injections. For the first time, it is worth choosing a small volume of oil solution - from 0.15 to 0.25 ml to make sure that your body tolerates subcutaneous injections well and the injection site is inflamed the next day.
If everything is fine, then you can try to increase the volume of the solution by 0.1 ml to a maximum of 0.5 ml (although most likely you will stop at 0.25-0.35 ml per injection). Usually, the dosage is divided into the required number of injections and injections are given every day. Of course, this can be used when your testosterone dosages are small - 125-250 mg, but if you decide to use a dosage of 500 mg or higher, then for sure it will cause you difficulties, because the number of injections will be too large and you will simply get tired of doing it.
Subcutaneous HCG injections
The second way to avoid intramuscular injections is to use HCG 2000-2500 IU per week, which will allow you to keep own testosterone level within reference values and avoid testosterone deficiency symptoms.
The form of application of HCG, although it is injectable, but the injections are made with a small insulin needle under the skin, which will not bring you any discomfort and stress. Such an injection is done very easily and does not require any special training other than following simple safety rules.
!!! We are ready to repeat this constantly: regardless of your goals - testosterone should be present in each cycle. You can't do cycles where there is no testosterone, otherwise you have a risk of getting a whole range of side effects and probably not getting any result.
CONCEPT 1️⃣ - SARMS MINIMALISM WITH SERMS TESTOSTERONE BASE
The purpose of this approach is, firstly, that for you it will be a “demo” cycle that will give you a result, although not as noticeable as it could be when using the second concept, after which you can understand whether you want to continue to try using PEDs or for example, follow natural training in the future. This is the case when you want to try the “Dark side”, but do it very carefully.
The advantage of SARMS is that they are not converted to estradiol and DHT, which significantly reduces the side effects associated with these hormones. But, as we know, these hormones also have their own positive effects on the body, so their indicators should always be within the normal range. The growth of estradiol and DHT is always associated with a large amount of testosterone, which we inject from the outside, because testosterone in this case is their source (prohormone).
We also know that SARMS, although not as significant as steroids, still inhibit the production of their own testosterone. As a result, after a while, when endogenous testosterone is suppressed, we are left not only without testosterone, but also without normal levels of estradiol and DHT. Low levels of these hormones lead to decreased libido and mood, general fatigue and lack of energy/motivation. In addition, anabolism is also reduced because both hormones are active anabolic agents. Low estradiol levels are problems with the lipid profile (cholesterol) and an increased risk of injury to the articular ligamentous apparatus, as well as a decrease in bone density. All this cannot be ignored, and we must somehow increase the level of these hormones during the SARMs cycle.
If you use very short cycles of 4 weeks, but there is a chance that you will not need any additional drugs to increase estradiol and DHT levels. But it is more accurate to say whether this is true or not - when taking blood tests for estradiol and total testosterone. This is what we recommend doing in week 4 to see how much SARMS has affected their levels. If the level of these hormones is below normal or close to it, we recommend starting an additional intake of one of these drugs.
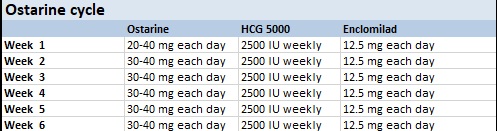
SARMs cycle design
SARMs, SERMs or HCG. All you need to do is to include some SARMs like Ostarine, S4 or RAD140 in your cycle and “test base” like Clomiphene or Enclomiphene. It is possible that during this cycle your HPTA will not be suppressed, which will make life easier for you later and save you from a lot of hassle. If Clomiphene doesn’t help you and your testosterone drops based on your bloodwork, then you can use HCG. It will work 100%. I also advise including HGH in your cycle. I believe that this drug is never superfluous, no matter what goal you set for yourself. It will give you tendon strengthening, get rid of some excess fat and, in theory, give you an additional increase in muscle mass.
HCG 2000-3000 iu/week. Gonadotropin, a drug that can quickly and effectively increase your own testosterone and estradiol levels, as well as DHT, respectively, by stimulating your testicles. The weekly dose should be selected based on blood tests, which we recommend taking a week after the first injection, making adjustments if necessary.
One commonly used option is to use clomiphene/enclomiphene during the SARMs cycle. Like gonadotropin, SERMs increases testosterone levels and, consequently, estradiol and DHT. SERMs are accepted daily or every other day. The dosage is usually the minimum required to maintain normal hormone levels. This is usually 25-50 mg of clomiphene or 12.5-25 mg of enclomiphene.
Purpose
Get an understanding of how your body responds to PEDs at the lowest dosages of the mildest drugs and decide whether to continue using them.
Advantages
You will not experience many side effects (most likely there will be none) and such cycle will be very easy to administer, without the use of additional drugs such as aromatase inhibitors and others.
It is possible that your own testosterone will remain at normal levels, and you will not need PCT or it will be very minimal and your testosterone will quickly return to norm.
The main advantage is that if you are satisfied with the result - you can repeat this cycle constantly for a long time, changing SARMs, dosages and duration- experimenting and studying your body’s reaction to all changes. Thus, within 2-3 years, you will get a good result and most importantly, you will not suffer from a significant drop in testosterone levels, as after regular cycles of anabolic steroids. Believe me- slowly and gradually, but surely and without hormonal pits- this is also a great option that can suit many. If I could turn back time, I would try this method.
Of course, you must understand that only your personal experience can confirm or deny the effectiveness of this concept. A lot depends on your individual characteristics. For example, even using minimal dosages, there will be people whose testosterone will still decrease very significantly.
For whom it suits
People who are not in a hurry, want to look good, feel healthy, but do not chase competitive bodybuilding titles and do not have the desire to become a mass monster. Your body over time can become very aesthetic, close to the body of athletes in the amateur nomination men’s physic. This is the body that most men want and this type of cycles may work for this goal…
An option of alternation with SERMs
We think it’s a very good idea to alternate 6-10 weeks of these light cycles with 6-10 weeks of SERMs during which you can raise your testosterone even above normal levels. In this case, you seem to be on TRT, but nevertheless, it is possible without suppressing your own testosterone levels (if the dosages of SARMs are not high).
Disadvantages
The result will be lower. In total, it will most likely be 50% of the result that you would get from classic anabolic steroids cycles, but this is safety fee.
CONCEPT 2️⃣ - A HARDCORE CONCEPT
How this concept differs from the previous one is that it is completely opposite in its essence. If in the previous version our approach was based on using the mildest drugs, trying to minimally interfere with the hormonal system in such a way that we would avoid significant suppression of our own testosterone and any side effects. The same cycle option is when you immediately use high dosages relative to what is usually used in your first cycle to achieve more significant results.
To be honest, we do not support this approach. We would not recommend doing this to anyone, but there are stubborn people who want everything at once- and I’d rather write a moderate version than they will inject everything into themselves.
PEDs:
Testosterone is always used, but the dosage will depend on the goals. We recommend using slightly higher dosages of testosterone if your goal is bulking and slightly lower doses relative to your second component in the stack if your goal is cutting. However, we will talk about this in more detail in the following chapters.
Other drugs are selected based on your goals. Mandatory use of HCG, aromatase inhibitors, and SERMs on PCT.
Purpose
The point is that in this case you do not try to be careful, but immediately use effective dosages that will bring you results. You will surely have some side effects and you can probably immediately assess whether you need it or not. There is nothing dangerous in this, but the first signs of gynecomastia, water retention, acne are the side effects to be expected, especially if you do not adhere to the aromatase inhibitor regimen and ignore blood tests.
Advantages
This approach makes it possible to progress as quickly as possible from the first cycle.
Long-term perspective
Whether this is the best option for a long distance – most likely not. I believe that you should always start with minimal dosages and light drugs, even if your goal is to become monstrously massive and there are many reasons for this.
You will be able to progress for a while without increasing the dosage from cycle to cycle, but after a couple of years, your dosages will most likely increase. The reason is that at medium dosages you will already stop growing, and to grow at high dosages you need to train very competently, which very few people can do. And often side effects in the form of increased estradiol and prolactin will not let you progress. As a rule, people who have chosen this path have a poor understanding of these processes.
For whom it suits
This choice can only be suitable for a person who has a sufficiently large theoretical experience in understanding PEDs, who is ready to try to apply this experience on himself, without additional caution.
But most often this path is chosen by those who are in a hurry to see themselves 20 kg more massive, bot particularly worried about side effects.
Disadvantages
As you have already understood, the main disadvantages are: the possible side effects, some administration complexity, as you would need to use additional drugs, mandatory blood tests and precise control of your hormones.
All this can be too difficult for a beginner. Also, after each cycle, PCT is waiting for you.
CONCEPT 3️⃣ - SOMETHING AVARAGE
In addition to these two opposing views on your first and subsequent cycles, there is also an intermediate option, which I will still refer closer to the first concept, but for people who still do not want a little more bust than SARMs can offer.
The only difference will be that instead of SARMs, you will use some of the mild anabolic steroids that we have listed above, as well as testosterone, but in minimal amounts to avoid using aromatase inhibitors or use them in minimal amounts. Of course, using anabolic steroids, even in minimal amounts, you will not avoid a decrease in your own testosterone and a subsequent longer PCT than if you were using SARMs.
As an example, I will give two options, one of them will be closer to the concept of minimalism, and the second to hardcore, but the second, like the first, I consider quite rational and acceptable.
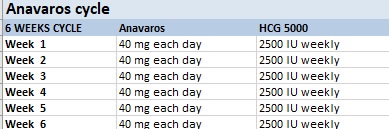
We took oxandrolone as an example, but you can choose any of the oral medications that we recommended above.
In the first option, you will use HCG as a testosterone base so that the level of testosterone in your blood does not turn out to be zero and you do not get the corresponding side effects due to the lack of testosterone, estradiol and DHT. Injections are carried out subcutaneously using small insulin needles, so this will not create any discomfort even for a person who has seen a syringe for the first time.
We recommend doing this cycle for about 6 weeks, because with each week it will be more difficult for you to keep your testosterone levels with HCG at normal values without increasing the dosage.
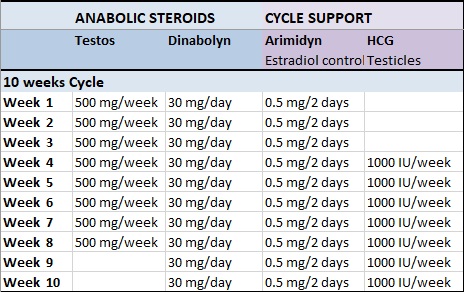
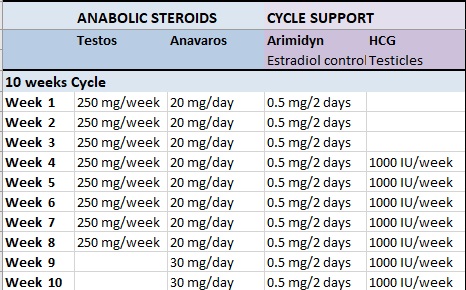
In the second option, we will use testosterone, and then this cycle will be a classic beginner steroid cycle. The dosage of testosterone that we offer is 250 mg (1 ml), which you can divide into smaller injections and do not intramuscular injections but subcutaneous (we talked about this above)
The advantage of this option is that you will use testosterone and the total dosage of anabolic steroids will be higher, therefore this fix will be much more productive. The other advantage is that it is possible to do it for more than 6 weeks without your testosterone in the blood decreasing. Of course, your endogenous testosterone will be reduced, but you won't feel it because your blood will have high levels of exogenous testosterone.
There is only one drawback to this cycle - your PCT will be a little longer than if you used the first option or the concept of minimalism with SARMs.
Leave a Comment