



It is typical for a person to lose up to 100 hairs daily, while the loss of a large amount of hair is already a pathology and leads to baldness: Changes in the immune status, endocrine diseases, functional disorders of the nervous system, chronic infection, genetic factors, changes in the rheological properties of blood, disorders of the peripheral vascular system and cerebral vessels, an imbalance of trace elements, etc. will be introduced to baldness. One of the main causes of alopecia is androgenization, an excessive amount of male sex hormones.
ANDROGENIC ALOPECIA
Androgenization is often the cause of baldness in men whose hair loss occurs initially in the form of a deepening of the hairline in the frontal-parietal regions, and later the appearance of a bald spot on the upper surface of the head.
Androgenic alopecia is caused by a decrease in the size of hair follicles under the action of androgens. Have you ever wondered why, in old age, all women have hair on their heads, while most men have terrible thinning and receding hairlines? Because of androgens. The main sex hormone in men is testosterone, while in women it is estrogen.
Because women have significantly less testosterone, they have significantly fewer androgens, and with significantly fewer androgens, they have minimal body hair growth, minimal hair loss from the head, and minimal masculinity in general.
On the other hand, testosterone levels are much higher in men, and this testosterone is metabolized by 5α-reductase in DHT, which can then bind to receptors in hair follicles. Men are much more likely to grow body hair, hair on the head is much more likely to fall out, and they develop muscular features.
According to The American Hair Loss Association: “Androgenetic Alopecia or common male pattern baldness (MPB) accounts for more than 95% of hair loss in men. By the age of thirty-five two-thirds of American men will experience some degree of appreciable hair loss, and by the age of fifty approximately 85% of men have significantly thinning hair.”
The relationship between baldness and the amount of male sex hormones was described by Hippocrates, who noticed that eunuchs never go bald. And only in 1940, American Dr. James Hamilton made a scientific conclusion that hereditary predisposition to elevated levels of sex hormones (especially dihydrotestosterone) is the cause of androgenic alopecia.
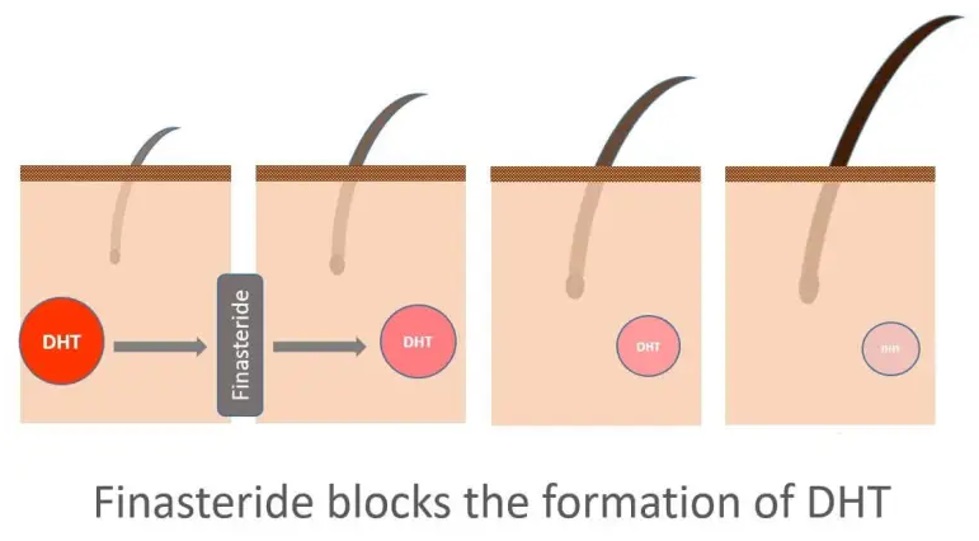
Testosterone is the main sex hormone in men and is partially converted by the enzyme 5α-reductase to DHT, which is much more dangerous to your hair than testosterone. Dihydrotestosterone (DHT) is an endogenous androgenic sex steroid and hormone that is a byproduct of its own testosterone levels. DHT has a much higher affinity for binding receptors in hair follicles than testosterone.
An excess of dihydrotestosterone or a high activity of the enzyme 5-alpha-reductase, which contributes to its formation from testosterone, leads to a gradual decrease in the vital activity of hair follicles (bulbs), consequently, thinning and hair loss. However, the degree to which this will happen individually affects your hair and will depend on factors: how much testosterone is contained in your body, how much of it is converted into DHT, on your sensitivity to androgens in hair follicles and on what hormones are circulating in your body.
GENETIC TESTING IN ANDROGENETIC ALOPECIA
A diagnostic test based on gene polymorphism is now available to predict the likelihood of developing androgenetic alopecia (53,56). This test can be useful for young patients concerned about hair loss, helping them decide on early treatment initiation.
In men, the test can forecast the risk of male androgenetic alopecia (MAA) by detecting a specific variation in the androgen receptor gene on the X chromosome. This variation affects how hair follicles respond to dihydrotestosterone, altering the hair growth cycle. A positive result indicates a 70% chance of developing MAA, while a negative result indicates a 70% chance of not developing it. This test serves as a screening tool to predict future MAA risk rather than as a confirmatory test.
STEROIDS AND ANDROGENIC ALOPECIA
For those who use excessive doses of exogenous steroids, the rate of miniaturization of hair follicles will increase, again, depending on how androgenic the compounds are, how much they are used, personal sensitivity to this particular androgen, etc.
Steroids with an appropriate genetic predisposition can accelerate baldness. Scalp receptors have a strong chemical affinity for dihydrotestosterone (DHT), so as with acne, it is primarily responsible for baldness as steroids are converted in the body to significant amounts of DHT. And here in the first place is injectable testosterone. As a result, it’s use, bald patches and general hair thinning occurs. This side effect is not reversible, hair restoration is excluded. It should be emphasized again that anabolic/ androgenic steroids do not automatically cause baldness on their own. But they can accelerate baldness in athletes predisposed to it.
As you can see, there are many high-level bodybuilders who completely lack the problem of hair loss, despite the fact that they most likely use large dosages of anabolic steroids. This proves once again that if you do not have a predisposition to baldness, you have nothing to fear. if you have men with alopecia in your family, then there is a chance that this side effect will not pass you by.
Scientists have found out that baldness is inherited on the maternal side, not on the paternal side. It has been established that baldness is transmitted along the X chromosome, that is, the maternal one. This means that if your mother's father was bald, it is more likely that you will also experience baldness.
FINASTERIDE – A PRIMARY TREATMENT OPTION
The 5-alpha reductase inhibitor finasteride blocks the conversion of testosterone to dihydrotestosterone (DHT), an androgen responsible for male-type hair loss (androgenic alopecia) in genetically predisposed men.
The 5-alpha reductase inhibitor finasteride blocks the conversion of testosterone to dihydrotestosterone (DHT), an androgen responsible for male-type hair loss (androgenic alopecia) in genetically predisposed men.
RESEARCHES
Finasteride is an FDA approved treatment for androgenic alopecia. Finasteride is a well-studied drug and its effectiveness in the treatment of baldness has long been proven by many clinical trials.
The results of phase III clinical trials involving 1879 men showed that oral administration of finasteride in a dose promotes hair growth and prevents further hair loss in a significant proportion of men with male-type hair loss. Hair counts in these men showed that 83% of patients treated with finasteride, compared with 28% of patients treated with placebo, did not experience further hair loss compared to baseline after 2 years. Therapeutic doses of finasteride are generally well tolerated. In phase III studies, 7.7% of patients treated with finasteride at a dose of 1 mg/day, compared with 7.0% of patients treated with placebo, reported treatment-related side effects. Most of the side effects were mild to moderate in severity
pubmed.ncbi.nlm.nih.gov/9951956
HOW IT WORKS
Its effect begins as the drug accumulates in the body, not earlier than after 3-4 months of administration. The maximum effect is observed after 2 years from the start of use. The effect of reducing the concentration of DHT is manifested only with constant medication. The withdrawal of the drug after a while will lead to the progression of the disease, so if you want to save your hair, then you should use finasteride on a regular basis while you use anabolic steroids.
As soon as finasteride is metabolized by your body, it will start to reduce the amount of DHT that circulates in your bloodstream. This means that your hair will be protected from the harmful effects of DHT just a few hours after you take your first dose of finasteride. On average, finasteride reduces the amount of DHT in your bloodstream by around 70 percent, which is enough to significantly slow down, stop or even reverse hair loss that’s caused by male pattern baldness.
THE FIRST 3 MONTHS
However, because it takes time for your hair to successfully make its way into the first phase of its natural growth cycle, you may not see any results right away. During the first few months of using finasteride, you probably won’t notice much of a change in your hair. Your hairline, crown and your general level of hair thickness will probably look exactly the same as normal, with no significant improvements.
This isn’t because finasteride isn’t working properly. Instead, the lack of visible progress during the first few months is simply because your hair needs to grow before results are obvious.
During the first few months, it’s important that you continue to use finasteride each day, even if you don’t notice any results. Rest assured that the medication is working properly -- it’s just too early for its effects on your hair to be visible.
6 MONTHS
Most of the time, early results from finasteride start to become visible after around three to six months of daily use. After taking finasteride for this amount of time, you might notice that your hair loss has slowed down or stopped, with no further visible thinning. You may also see improvements in your hair, particularly in areas such as your hairline and crown.
12 MONTHS
After taking finasteride consistently for 12 months, you should see further improvements in your hair that build on your progress from months three to six. Most studies on finasteride show significant, measurable increases in hair count, thickness and reduction in the hair loss process after 12 months of treatment.
For example, a 1999 study published in the Journal of the American Academy of Dermatology found that men who used finasteride over a period of one year showed a significant increase in hair count in the frontal scalp (hairline) area. Clinical trials have also found that about 65 percent of men treated with finasteride show some degree of increased hair growth after 12 months.
Since everyone’s hair is slightly different, there are no precise results that you should expect at the 12-month mark. You may have a modest increase in hair growth that you can see when you brush your hair or look in the mirror, or significant improvements that are easy to notice.
LONG-TERM USING
Finasteride keeps working after the 12-month mark, with most research showing that men who use the medication for the long term continue to see a reduction in hair loss and improved hair growth.
A study from 2003 looked at the results of finasteride over two years. The researchers found that men who used finasteride displayed a 14 percent improvement in hair count after one year of treatment, as well as a 16 percent improvement after two years.
An even longer study from Japan looked at the effects of finasteride on hair loss over five years of treatment. The researchers noted that 99.4 percent of men who used oral finasteride tablets during the study period showed improvements.
Put simply, the long-term effects of finasteride appear to be the same as those that occur in the short term -- a reduction in hair shedding, improved hair growth and noticeable improvements in hair thickness and scalp coverage.
After you get results, don’t stop using finasteride. Keep taking finasteride, even after you see results. If you stop taking finasteride, your DATA levels will rise and your hair loss may start to worsen again.
DOSAGES
The traditional treatment regimen involves taking 1 mg of Finasteride daily, but recent studies say that just 0.2 mg of finasteride per day has exactly the same efficacy, which significantly reduces any risks of side effects
pubmed.ncbi.nlm.nih.gov/10495374
RESULTS (BEFORE AND AFTER)











After 2 years on finasteride 1.67mg/day and minoxidil solution 5% PM

After 12 months on finasteride 1.25mg/day

About 1 year on finasteride 1.25mg/day PM

The results are taken from the clinic's website bernsteinmedical.com
INTERACTION WITH OTHER ANABOLIC STEROIDS
Testosterone is the only anabolic steroid that is converted to DHT by 5-alpha reductase. Most anabolic steroids do not interact with 5-alpha reductase at all. Some anabolic steroids, such as Primobolan or oxandrolone, have higher anabolic activity in the body with lower levels of androgenic activity and do not interact with 5-alpha reductase at all. Due to their low androgenic activity, they are considered much safer for hair. This applies to a variety of anabolic steroids such as: methandienone, turinabol, stanozolol, oxymetholone, proviron. These drugs are much safer for hair relative to testosterone.
There are several other steroids that do not interact with 5-alpha reductase, but still cause hair loss, such as trenbolone. Therefore, even if you use finasteride during the testosterone plus trenbolone cycle, unfortunately, taking it cannot completely eliminate the negative effect on the hair, although it will be much lower than without using finasteride. Drostanolone is considered the king of negative effects on hair follicles among steroid users. Despite the fact that the drug itself does not have a large number of side effects and is considered quite mild.
Other steroids that interact with 5-alpha reductase are converted into unique metabolites with their own individual anabolic and androgenic activity. For example, boldenone can be converted to dihydroboldenone (DHB) using 5-alpha reductase. Nandrolone can be converted to dihydroandrolone (DHN) by 5-alpha reductase. Each of the two metabolites DHB and DHN has its own unique anabolic and androgenic activity and cannot be compared with DHT.
There is an example of steroids that are better not to use together with finasteride and such examples are nandrolone. Despite the fact that nandrolone is not a steroid with a high level of androgenicity compared to testosterone, its metabolite DHN, which is formed when interacting with 5alpha reductase, is even less androgenic than the parent hormone. If we use finasteride, it turns out that most of the DHN stops forming and the amount of nandrolone in the blood increases, and this somewhat worsens the situation for the hair due to the higher androgenic activity of nandrolone compared to DHN. Conclusion - when using finasteride together with nandrolone, the overall androgenic effect increases.
The general concept to keep in mind is that all steroids have their own individual level of anabolism and androgenicity in the tissues. The more androgenic the steroid, the more effect it has on the hair follicles. Regardless of whether the steroid is a 5-alpha-reduced metabolite or a parent hormone, ultimately, they are all still steroids with their own anabolic and androgenic effects on body tissues, and this should be taken into account.
Finasteride actually protects you from the negative effects on hair follicles when using testosterone, which turns into DHT. Finasteride has no other ways to protect against hair loss. So, finasteride cannot protect you from hair loss if you use other anabolic steroids. On the other hand, testosterone (or rather its metabolite (DHT) is most likely the most aggressive agent regarding the effect on hair. Therefore, if your cycle consists of testosterone and other anabolics and you will use finasteride, it will in any case have a positive effect on your hair and protect against baldness. Of course, it is better for you to avoid using nandrolone (we announced the reason earlier) as well as trenbolone and drostanolone. Other popular steroids have a much less mild effect on your scalp hair.
MYTH – LESS DHT MEANS LESS MUSCLE
There is a myth that says that a decrease in the level of DHT in the blood can somehow reduce the results of the muscle mass cycle, but this is not the case at all and in some sense the opposite. DHT has such a low selectivity to anabolic tissues that it is one of the few steroids whose androgenic level is several times higher than that of anabolic. In short, DHT does not help build muscle mass.
In a study conducted to determine whether taking dutasteride (a drug that reduces DHT even more effectively than finasteride) would increase muscle mass, those who received the drug had results similar to those of the control group who did not receive dutasteride treatment; this means that reducing DHT levels did not have a significant anabolic effect on growth muscles
pubmed.ncbi.nlm.nih.gov/22396515
Even after dutasteride almost completely reduced the participants' DHT levels, they had no difficulty at all in growing muscles in response to increased doses of testosterone. In fact, it can be argued that inhibition of 5-alpha reductase can promote supraphysiological muscle growth due to a higher ratio of testosterone and DHT. A decrease in DHT levels leads to an increase in testosterone levels, which directly increases anabolic processes.
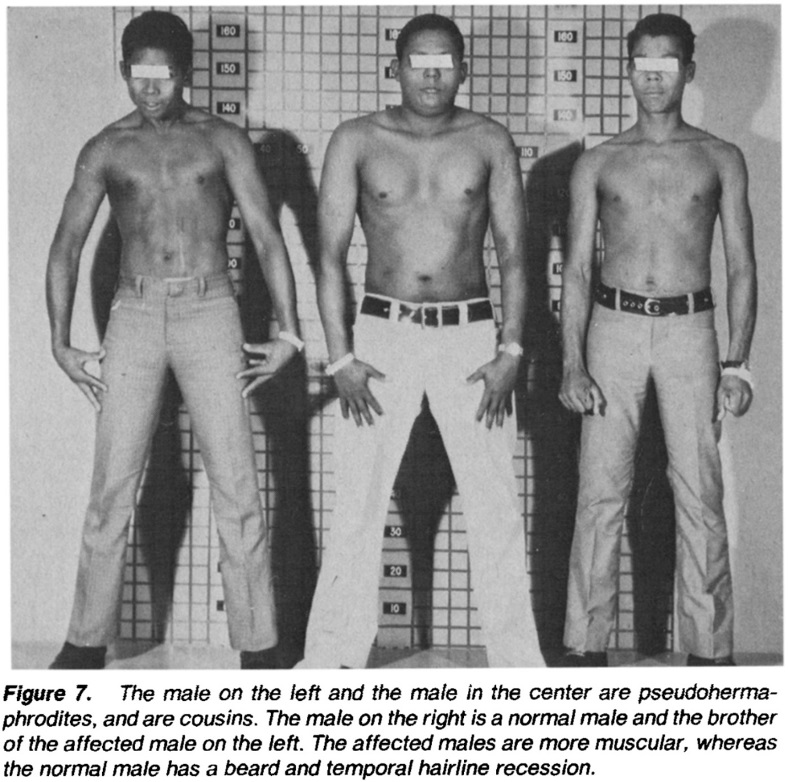
This is evident in pseudohermaphrodites, which are inherently deficient in 5-alpha reductase due to genetic mutations. In this particular study involving brothers with different levels of DHT, a man with 5-alpha reductase deficiency had a decrease in sexual development during puberty, but he also had more muscle mass than his brother. In the image below, the man on the left has a deficiency of 5-alpha reductase, while his brother on the right does not have this deficiency.
FINASTERIDE INCREASES TESTOSTERONE
When you suppress the conversion of testosterone to DHT with finasteride, you are left with more circulating testosterone because its conversion to DHT is largely suppressed by finasteride. The official brochure from Propecia's manufacturer, Merck, says that average testosterone levels in the blood have increased by about 15%.
PROSTATE ENLARGEMENT
Doctors use finasteride to treat prostate hypertrophy. Finasteride may improve symptoms associated with such as decreased and painful urine flow. It provides better symptomatic treatment than alpha-1 blockers such as tamsulosin, but symptom relief comes slower (treatment with finasteride may take six months or more to determine the therapeutic outcome). In long-term studies, finasteride, but not alpha-1 inhibitors, reduced the risk of acute urinary retention (-57% at 4 years) and the need for surgery (-54% at 4 years). When you stop taking the drug, changes in the prostate are restored within 6-8 months.
RU58841
RU58841 is a nonsteroidal antiandrogen that was originally developed in the 1980s by the French pharmaceutical company Roussel Uclaf, after which it got its name. By suppressing the harmful effects of DHT on hair follicles, RU58841 helps preserve existing hair and prevents further hair loss. There are studies that prove the effectiveness of this drug. RU58841 is applied topically to the scalp, just like minoxidil.
HOW IT WORKS
Despite the fact that finasteride significantly protects the hair, however, in order to protect your follicles completely, finasteride alone may not be enough. The fact is that although testosterone is much less androgenic than DHT, it can still have some effect on your hair. To completely avoid this effect, you need to block the androgen receptors on your head. This can be done with the help of topical androgens that directly locally affect the scalp. The most popular topical antiandrogen is RU58841. On the Internet, a very large number of people use this tool and have excellent results. Of course, RU58841 has not yet been approved by the FDA, unlike finasteride and does not have such a large evidence base in the form of scientific research, but still both animal and cell studies and the practice of many people allow us to say with confidence that this drug is also extremely effective in combating androgenic allopecia.
By binding to androgen receptors, RU58841 causes antiandrogenic effects in hair follicles and provides an additional level of protection when necessary, or as an independent form of monotherapy, if this is sufficient without reducing the level of androgens in the blood.
For some people, finasteride monotherapy will be enough to prevent hair loss for a couple of decades, but residual DHT levels and a surge in testosterone will continue to affect the follicles and eventually win. The optimal prevention is the use of antiandrogens in conjunction with finasteride and the addition of minoxidil.
RESEARCHES
In the study, finasteride was compared with RU58841 to find out which one is more effective for preventing hair loss. The short-tailed macaque has proven to be a suitable biological model for human androgenic alopecia, as it has hereditary signs of baldness, in many ways similar to androgenic alopecia in humans.
RU58841 was applied either in a 5% solution, or in a 0.5% solution, or simply a placebo solution containing no RU58841 was used for 6 months on the scalp of 10 short-tailed macaques.
A 5% solution was applied to 4 out of 10 bald short-tailed macaques, a 0.5% solution was applied to 3 out of 10 bald short-tailed macaques, and a solution without RU58841 was applied to 3 out of 10 bald short-tailed macaques. The generally accepted RU58841 dosing protocol usually involves applying a 5% solution to areas affected by androgenic alopecia, so this study was consistent with what we would like to see. 10 bald short-tailed macaques were administered finasteride orally at a dose of 1 mg/kg per day for 6 months. Another 10 bald short-tailed macaques were also given placebo orally.
Skin biopsies for micromorphometric analysis (folliculogram) were taken after 6 months in macaques treated with finasteride and 4 months in macaques treated with RU58841. The number of anagenic follicles (hairs in the active growth phase) and downy follicles (short, thin and barely noticeable hairs) enlarged to the final size was compared with those at the pre-treatment stages. The number of anagenic follicles increased by an average of 88% when taking finasteride. The number of anagenic follicles increased by an average of 103% when taking the 5% drug RU58841. The growth of soft follicles to the final size (thick, strong, pigmented hair that is fully mature) with the use of finasteride was 12%. The growth of soft follicles to the final size when using 5% of the drug RU58841 was 26%.
The 0.5% solution of RU58841 had practically no effect. As expected, the placebo with finasteride had no effect. A 5% solution of RU58841 caused the greatest hair growth after just 2 months of treatment.
Although Finasteride significantly reduced the level of DHT, the remaining DHT produced by the type I 5α-reductase isoenzyme still contributed to the miniaturization of hair follicles. Since both testosterone and DHT bind to androgen receptors, a locally sufficient dose of an “AR blocker” (local antiandrogen) appears to suppress follicle regression caused by testosterone and DHT more effectively than inhibition of 5α-reductase.
infona.pl/resource/bwmeta1.element.elsevier-5d8b8e9a-87d8-3665-a251-1f766eb8cef1
DOSAGES
A dosage of about 50 mg of the active substance per day is usually used. The amount of ml will depend on the concentration of the substance per 1 ml used by the manufacturer. This is usually 50 mg/ml. That is, if you want to use 50 mg per day, then it will be 1 ml for you.
MINOXIDIL
Minoxidil promotes hair growth by prolonging the anagen phase, increasing the follicular size and stimulating the growth of hair follicles at rest. The effective effect of the drug on the restoration of the scalp, reduction of hair loss was noted. It is not a growth stimulant, does not affect the hormonal background of the body as a whole.
It was first used to treat severe forms of arterial hypertension (high blood pressure) in the 1970s as an oral medication. It causes vasodilation by opening potassium channels. It was noticed that when ingested, patients experienced increased body hair growth - hypertrichosis, and this side effect developed in 24%-100% of patients. Interestingly, hypertrichosis was observed with greater frequency and at lower doses in women than in men. However, it was not possible to associate this hypertrichosis with the effect on the endocrine system - no endocrine pathologies were observed with prolonged oral administration.
Hair growth caused by minoxidil was not described in the dermatological literature until 1979. In the same year, tablets containing minoxidil, Lonitene, were approved by the FDA for the treatment of hypertension. And since that time, dermatologists have begun to investigate its effectiveness in hair loss.
RESEARCHES
The effectiveness of minoxidil in relation to hair restoration in androgenic alopecia has been convincingly proven in many randomised clinical trials with double-blind and placebo control, which served as a reason to consider minoxidil a basic drug for the treatment of male and female hair loss.
ncbi.nlm.nih.gov/pmc/articles/PMC6691938
The results of a randomized placebo-controlled 16-week trial using 5% minoxidil foam showed that 70.6% of 180 patients had an increase in hair growth compared to 42.4% of 172 participants using placebo.
HOW IT WORKS
One of the main hypotheses is based on its ability to activate potassium channels and lead to an increase in DNA synthesis in follicle cells. Minoxidil stimulates the ATP-sensitive potassium channel, which eventually leads to vasodilation. Dilated blood vessels can deliver more oxygen and nutrients to the hair follicles and thus promote hair growth.
Minoxidil can also reduce the expression of the interleukin-1 alpha gene and, thus, can reduce microinflammation of perifollicules by inhibiting inflammatory mediators such as interleukin-1 alpha, which promotes hair growth.
Minoxidil can inhibit the expression of the type II alpha-reductase 5 gene and, thus, can act as an antiandrogen and promote hair growth.
Minoxidil can also induce the Wnt/b-catenin signaling pathway by stimulating the release of VEGF in the cells of the dermal papilla, which leads to the regeneration of hair follicles.
Minoxidil may promote hair growth by playing an important role in the anagen phase. The drug may cause the early onset of the anagen phase by enhancing the synthesis of DNA in the anagen bulb. Furthermore, minoxidil may have the potential to lengthen the anagen phase, shorten the telogen phase, or influence both of these hair growth phases. An experiment on a rat model showed that topical minoxidil preparation did not extend the anagen phase but reduced the telogen phase duration. Another study conducted on stump-tailed macaques demonstrated that the application of topical minoxidil solution contributed to the regulation of both the telogen and anagen phases, ultimately leading to an increase in hair follicle size.
Minoxidil itself is a stable but inactive component. Inside the hair follicle, minoxidil does not act directly, it turns into minoxidil sulfate, a more active derivative that stimulates hair growth.
The conversion of minoxidil into sulfate occurs with the help of sulfotransferase enzymes, which are found in the cells of the hair follicle. It was also revealed that there are individual differences in the level of sulfotransferase in the skin. Patients who responded better to the use of minoxidil had higher levels of sulfotransferase activity in the skin, in patients who did not respond to treatment, sulfotransferase activity was minimal.
Cosmetically acceptable hair growth is ensured by the effect of minoxidil on hair thickening, reducing hair loss and increasing hair density. In accordance with international AGA treatment standards, minoxidil is prescribed externally to women and men in concentrations of 2 and 5%, respectively.
To evaluate the effectiveness of treatment, it is necessary to regularly apply a lotion, usually containing minoxidil, twice a day for at least six months. After topical application, minoxidil accumulates in the upper layer of the epidermis, and then gradually spreads throughout the body.
It should be understood that minoxidil improves hair growth, but does not eliminate the problem itself, that is, it does not reduce the amount of DHT in your blood, which means that with minoxidil you can slow down hair loss, but not stop it. Therefore, the most effective combination is the combined use of finasteride/antiandrogens and minoxidil.
ORAL MINOXIDIL
In recent years, oral administration of low doses of minoxidil for hair loss has become increasingly popular. Although this drug is not approved by the FDA for the treatment of hair loss in men and women, clinical studies show promising results in the treatment of various types of hair loss, including male and female type hair loss (androgenic alopecia), focal alopecia, telogen loss, traction alopecia and hair loss caused by chemotherapy.
Studies show that oral administration of minoxidil is at least as effective in stimulating hair growth as topical application of minoxidil, and can be used with poor tolerability of topical application of minoxidil
pubmed.ncbi.nlm.nih.gov/32622136
pubmed.ncbi.nlm.nih.gov/34159872
Minoxidil can lower blood pressure, so taking it together with other antihypertensive drugs can lead to excessively low blood pressure (hypotension).
DOSAGES
The efficacy and safety of 5% minoxidil in the form of foam for topical application 2 times a day was shown in a study conducted in men with androgenic alopecia. Oral minoxidil dosages is from 2.5 to 10 mg once a day. Dosages of 5 mg have previously been studied, but there are studies that suggest that 2.5 and 1.25 mg are just as significantly effective
pubmed.ncbi.nlm.nih.gov/33682223
Minoxidil for androgenetic alopecia is a drug for long-term use. When choosing this drug, it is necessary not to forget that when canceling treatment, the positive changes obtained with the use of minoxidil will go away 4-6 months after discontinuation of use, this phenomenon is called the "withdrawal syndrome" of minoxidil.
ONCOLOGY AND BALDNESS
Minoxidil can also be used in other cases when it is necessary to give the hair a boost to growth, for example after antitumor therapy. In 25-30% of cancer patients, as a result of antitumor therapy, persistent alopecia is observed, which is defined as incomplete hair growth 6 months after cytotoxic chemotherapy or the start of endocrine therapy, which can have a particularly serious impact on their quality of life.
Chemotherapy-induced hair loss affects 65% of cancer patients, and the psychosocial impact on these patients can be severe; it can include anxiety, depression, negative body image, decreased self-esteem and feelings of well-being. In some cases, the fear of hair loss as a result of cytotoxic chemotherapy can be so strong that patients may choose less effective cancer treatments that do not have this side effect, or refuse treatment altogether.
A recent retrospective study by Dr. Lacutour and his colleagues, presented at the ASCO Annual Meeting in 2022, offers alopecia sufferers an effective and inexpensive means to restore hair growth. The study examined whether cancer patients who have frontal and occipital alopecia after cytotoxic or endocrine therapy may benefit clinically from oral administration of low doses of minoxidil, an older drug that has historically been used in higher doses to treat hypertension. The study involved 216 women, most of whom (170) had breast cancer. A total of 31 women received chemotherapy alone, 65 received endocrine monotherapy and 120 survivors received chemotherapy followed by endocrine therapy. The results of the study showed that after 3 months of daily oral administration of minoxidil at a dose of 1.25 mg, the average percentage change in hair density was 20.4% in patients with frontal alopecia and 21.4% in patients with occipital alopecia. Similar results were obtained with respect to follicle density: 22.5% in patients with frontal alopecia and 20.9% in patients with occipital alopecia. None of the study participants stopped therapy due to undesirable effects.
Hair growth usually begins within 2-3 months after completion of chemotherapy. Thus, by about the fourth month in surviving patients, the scalp should be covered with hair about an inch and a half long. This discovery means that those who receive minoxidil orally in low doses will have about 20% more scalp hair, which is very important. Minoxidil for oral use contains the same active ingredients as the remedy for external use, but we found that people do not like to apply anything to the scalp every evening. The product for external use can cause dryness and itching of the scalp, so many people stop using it over time.
OTHER TREATMENT OPTIONS
You need to keep in mind that if you have already started baldness, then you will have to use one or more remedies that you will use to fight against baldness for the rest of your life. If you stop using them, then all your hair that should genetically fall out will fall out.
KETOCONAZOLE SHAMPOO
There is debate about whether this drug is an effective antiandrogen that affects hair follicles, and whether it has any effect at all. There is a lot of unofficial data confirming that it is useful and has antiandrogenic properties also for the scalp. Ketoconazole shampoo is not particularly risky, it is sold without a prescription, and it can be purchased without a doctor's prescription. There is no significant difference in the effectiveness of ketoconazole shampoos containing 1% and 2% solution. Keep in mind that this will most likely not be enough as monotherapy if you have even severe hair loss. However, if you are just starting to worry about hair loss or just taking care of your hair in general, sometimes this can be enough to stop the first signs of hair loss, and it is an excellent hair loss prevention tool. You may not need to use RU58841, finasteride, minoxidil and other drugs at once, if you do not have aggressive hair loss, start with shampoo.
Later, other stronger drugs will appear in your arsenal if you need them. If you do not have pronounced hair loss, buy a shampoo with ketoconazole and see how it affects the amount of hair loss. If you manage to get the situation under control with a good ketoconazole shampoo, then you're in luck. If not, then you will probably need something more intense, such as a real 5 alpha reductase inhibitor or a local antiandrogen. However, your situation may differ, since each person has their own individual genetic predispositions, hormonal background, the amount of hair to work with, and many other individual factors.
DUTASTERIDE
Unlike finasteride, the drug suppresses the activity of 5α-reductase isoenzymes of types 1 and 2 (finasteride is only type 2) which makes this medicine stronger, but at the same time carries a much greater number of side effects.
!!! That is why we strongly do not recommend using this drug.
SAW PALMETTO
This supplement is not a placebo; it does have an effect, albeit a modest one. It notably benefits urination. There's also a possibility that it might influence DHT (dihydrotestosterone), though the impact is relatively weak. If there are significant issues with elevated PSA levels, DHT increase, and prostate gland enlargement, finasteride is recommended. Saw palmetto, the supplement in question, can be used either in combination with finasteride or as a preventive measure.
ORAL ANTI-ANDROGENS
Oral anti-androgens (e.g., spironolactone, cyproterone acetate) have been widely used to treat women with androgenetic alopecia. However, these are contraindicated in men due to its feminization effects
SUPPLEMENTS
Traditionally, in the complex therapy of patients with hair pathology, metabolic complexes containing amino acids, pantothenic acid, biotin and their combinations, as well as a combination of L-cystine and pantothenic acid (CYP complex) are commonly used.
GROWTH FACTORS (PRP THERAPY)
A variety of growth factors and cytokines influence the growth and development of hair follicles. Using these growth factors to stimulate hair growth, either topically or subcutaneously, is a potential therapeutic target. Preliminary studies in animal models have shown positive results. A double-blind Phase I clinical trial was conducted to assess the safety of a bioengineered non-recombinant drug derived from human cells, containing follistatin, keratinocyte growth factor (KGF), and vascular endothelial growth factor (VEGF), to evaluate its effectiveness in stimulating hair growth. Twenty-six people participated in the study, and none experienced adverse reactions to a single intradermal injection. Statistically significant growth in total hair count continued a year later.
Platelet-rich plasma (PRP), derived from whole blood, can be used to obtain growth factors and stimulating mediators. PRP is also available as a standalone treatment for alopecia, with recent data indicating positive hair regrowth with minimal side effects. It is believed that PRP stimulates hair growth by enhancing follicle vascularization, inhibiting apoptosis, and thereby prolonging the anagen phase and promoting a quicker transition from the telogen phase to the anagen phase.
PRP therapy, or platelet-rich plasma therapy, is a hair loss treatment in which PRP from the patient's own blood is injected via microinjection. During the procedure, 25 ml of blood is drawn from a vein and centrifuged to prepare the PRP injection. The extracted PRP is then injected into specific points on the scalp after local anesthesia. Minimal pain is felt only if the patient's skin is particularly sensitive. About three to four months after the first PRP procedure, hair begins to grow, and the treatment results start to become noticeable. During and after the PRP procedure, platelets release growth factors that are responsible for the hair growth cycle. PRP activates hair follicle division, and the effects of PRP hair therapy become more noticeable after each session.
It is recommended to repeat PRP therapy for hair loss every 2-3 months, and the number of PRP sessions is determined by a medical specialist who assesses the causes of hair loss, intensity, contraindications, and other treatment-related factors. This procedure is available at many medical centers.
DERMAROLLING
Dermarolling is also highly effective, a procedure during which a roller equipped with mini-needles rolls over the surface of the skin. All these products have a fairly high usefulness and can be used in conjunction with finasteride, which can significantly increase the effectiveness of the application.
There are also studies that confirm that dermarolling, which is used together with minoxidil, improves the effectiveness of minoxidil
pubmed.ncbi.nlm.nih.gov/30886475
HAIR TRANSPLANTATION
It is believed that the hair follicles that are located on the back of the head do not have DHT receptors, so they never fall out. Hair transplantation is done in such a way that hair from the back of the head (and other areas where there are no DHT receptors, for example, from the beard) is transplanted to balding areas.
With the help of modern technologies, it is possible to reliably ensure the survival rate of a transplant exceeding 90%. Transplantation of follicular units can give very good results, but the success of the operation depends on careful selection of patients and the qualifications of surgeons. The hair density on the donor site should be optimal, and the correction of frontal baldness shows better results than the correction of the crown, where the disease tends to progress even after transplantation.
The patient's expectations should be realistic, he should know that the final result can be seen only after several sessions, after 5-6 months. In addition, the patient should be aware that temporary hair loss may occur after transplantation. As with any surgical intervention, it is necessary to take into account the risk of complications such as erythema, crusts and swelling, more serious infections, bleeding and scarring.
The disadvantages of hair transplantation are increased time and labor costs, which leads to increased costs for the patient. The transplanted hair, apparently, immediately after administration, passes into the resting phase of telogen. Thus, the results of surgical intervention can be adequately evaluated at least three months after the operation. There is always a certain degree of transplant failure. Dead grafts can be caused by various reasons, including the skill of the surgeon, the density of the graft placement, careless handling of the grafts and their preparation, as well as the drying of the grafts while waiting for the transplant.
TRICHOPIGMENTATION
This procedure is based on the technology of introducing pigment into the upper layers of the scalp with a special thin needle, which allows you to simulate the appearance of hair follicles on the scalp or individual hairs. Similar technologies are used by cosmetologists for women for eyebrows and are called permanent makeup. The specialist manually draws each hair, taking into account the growth line, color and density of the hair, so the result looks as natural as possible.
Of course, this cosmetic procedure has nothing to do with your real hair, but in some cases it can help. Firstly, in cases where your scalp is completely bald and you will no longer be able to restore your hair, or in the case when you have tried all the methods but you still lack hair density.
After this procedure, you can not wash your hair for 4 days and exercise for 4 days.

Before and after trichopigmentation
CONCLUSION
- If you want to do prevention and you do not have any signs of hair loss, then use shampoo with ketoconazole.
- If you notice the first signs of hair loss, your hair becomes lighter and thinner, your hairline goes up in front, then you can start adding products that slow down the effect of androgens on your follicles. You can start with a single remedy, for example, it can be RU58841 or finasteride and track the result. If the hair loss has stopped, then for now you can continue monotherapy.
- If monotherapy has reduced the effectiveness, you can add a second remedy. The combined use of RU58841 every day and 0.2 mg of finasteride per day are much more effective than both drugs separately.
- Add to this bundle a drug that improves hair growth - minoxidil (topical or oral version of the drug).
- To improve the effectiveness of RU58841 and topical minoxidil, you can start using a dermorller.
- If the situation has gone too far, then you can do one or more hair transplants. This will increase the density of hair in the places where they have fallen out, replacing it with hair from the back of the head that does not have androgen receptors.
- If hair transplantation has not solved this problem, you can improve the aesthetic appearance with the help of trichopigmentation. This is a much cheaper and simpler procedure, but it can significantly correct the appearance.
СOMBINED THERAPY
In an open, randomized, parallel-group study comparing the efficacy of various medications used as monotherapy or combination therapy (finasteride alone, finasteride with 2% topical minoxidil, topical minoxidil alone, and finasteride with ketoconazole shampoo), it was found that finasteride combined with either topical minoxidil or ketoconazole showed significantly better hair regrowth compared to finasteride monotherapy, with no difference in the incidence of side effects. This suggests that combining medications with different mechanisms of action enhances their efficacy.
Leave a Comment