Often beginners do not want to do their first cycle using anabolic steroids and especially injectable drugs, choosing oral SARMs because they have a milder effect than anabolic steroids. This way has its advantages and disadvantages, which we will discuss below.
What is SARMS
Selective androgen receptor modulators (SARMs) are a class of non-steroidal androgen receptor ligands that bind androgen receptors and exhibit tissue selective activation of the androgen receptor. SARMs have a selective anabolic effect on muscle and bone and were originally synthesized to treat muscle wasting, osteoporosis and breast cancer.
SARMs have almost the same effects as androgenic steroids, but they are much more selective and gentler. It is due to their selectivity that they are considered safer to use and have become popular among beginner athletes. SARMs are considered an alternative to steroids with reduced androgenic properties.
SARMs were created with an idea of producing a compound with zero or near zero androgenic activity (so as not to effect the prostate, skin and other organs) and with high anabolic activity in skeletal muscle tissue due to a direct connection to the androgen receptor. Therefore, SARMs are substances with high anabolic activity, low or no androgenic and estrogenic effect, which leads to much fewer side effects than with the use of anabolic steroids.
Mechanism of action
Selective androgen receptor modulators (SARMs) are drugs that can exert varying degrees of both agonistic and antagonistic effects on androgen receptors in different tissues. Their action can be understood by considering the selective estrogen receptor modulators (SERMs) that preceded them. Widely used to treat breast cancer, tamoxifen acts as an antagonist in the breast, an agonist in the bones, and a partial agonist in the uterus. The tissue-specific effects of these drugs are what make them attractive, as they can be tailored to treat specific diseases while minimizing side effects.
The main laboratory experiments were aimed at studying and optimizing the pharmacodynamic and pharmacokinetic properties of SARMs according to their desired site of action. SARMs have been chemically engineered to more specifically target androgen receptor function in certain tissues, minimizing side effects. The regulatory environment of each tissue allows SARMs to be relatively tissue specific.
Shortly about SARMs
● Suitable for beginners as well as advanced athletes who want to try something new
● SARMs are a safer alternative to anabolic steroids
● SARMs increase strength and muscle mass, strengthen bones and burn fat, but their effects is more subtle than that of anabolic steroids.
● SARMs have far fewer side effects (most often no side effects at all), so they are great for those who are ready to get a more moderate, but in any case, pronounced result, while minimizing all side effects.
● Each SARM works slightly differently from the other, so everyone should find their own drug that works best on it.
● Dosages for SARMs are individual in nature depending on the goal, gender and level of the athlete.
● After SARMs it still requires PCT with Enlomilad or Nolvados, but the recovery of one’s own testosterone is much faster because SARMs suppress it much less.
● You will usually take SARMs with one of the following: HCG, Enclomilad, Nolvados,
● Testosterone to ensure that your blood testosterone levels are high enough to support important bodily functions.
● During and/or after a SARMs cycle, it is advisable to take supplements such as NAC and TUDCA to support the liver.
SARM Cycle
Most often, this concept is suitable for the first cycle. The purpose of this approach is, firstly, that for you it will be a “demo” loop that will give you a result, although not as noticeable as it could be when using the second concept, after which you can understand whether you want to continue to try using PEDs or for example, follow natural training in the future. This is the case when you want to try to touch the forbidden fruit, but fearing the consequences, do it very carefully.
All you need to do is to include some SARMs in your cycle and test base like Clomiphene or Enclomiphene. It is possible that during this cycle your HPTA will not be suppressed, which will make life easier for you later and save you from a lot of hassle. If Clomiphene/Enclomiphene doesn’t help you and your testosterone drops based on your bloodwork, then you can use HCG. It will work 100%. I also advise including HGH in your cycle. I believe that this drug is never superfluous, no matter what goal you set for yourself. It will give you tendon strengthening, get rid of some excess fat and, in theory, give you an additional increase in muscle mass.
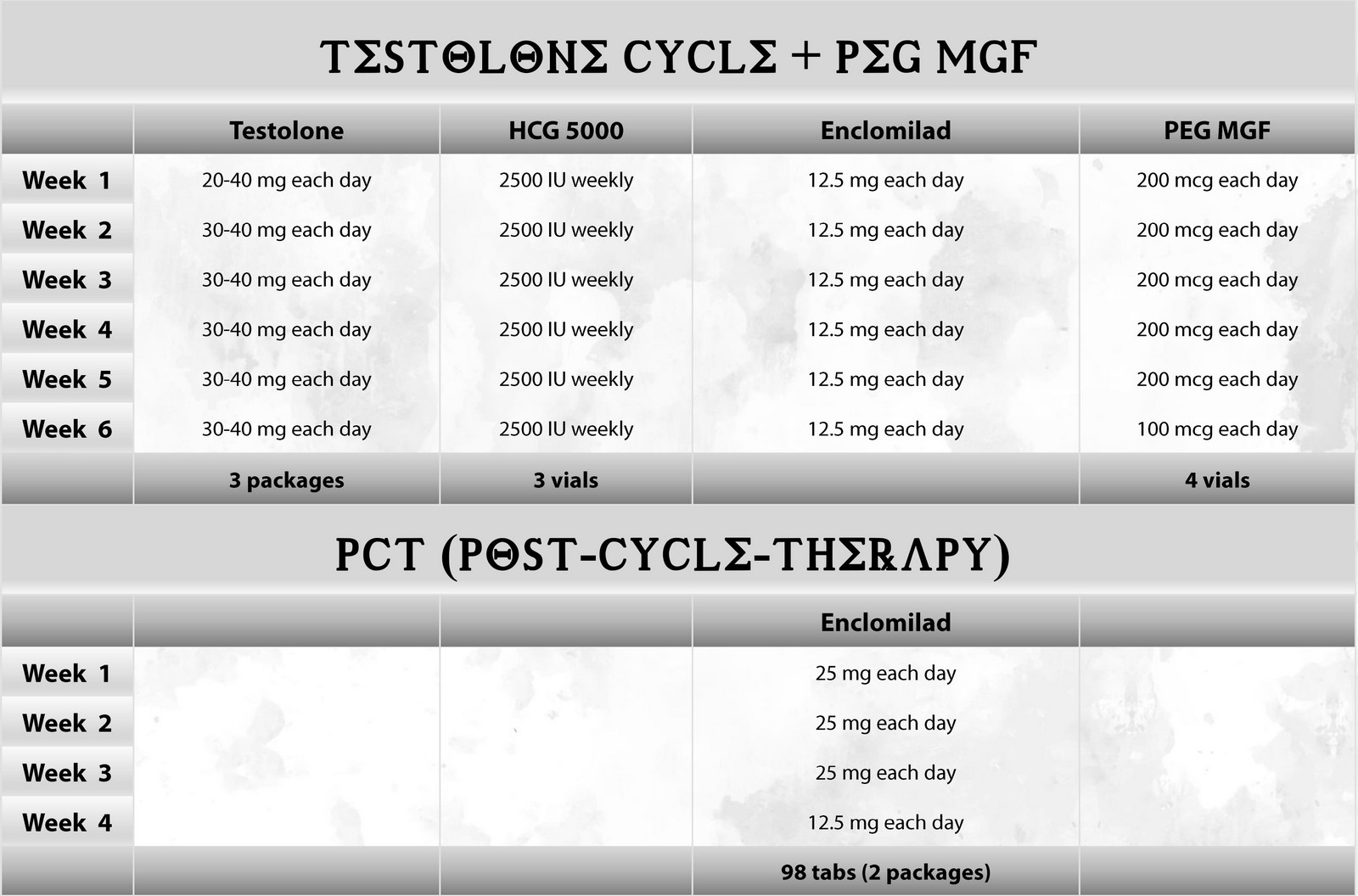
But in this cycle, we offer double support for your testosterone. In this case, you avoid intramuscular injections of testosterone, but with the combined use of Enclomiphene and HCG - you get a greater chance that your testosterone will be high enough to avoid side effects associated with low testosterone and estradiol levels.
Most likely, you will not be able to keep your testosterone for very long, so the cycle is limited to six weeks.
In 6 weeks, your own testosterone at the average (indicated in the table) dosages probably will not completely decrease yet. At this time, you will also use medications that will help it stay at normal values.
Purpose
Get an understanding of how your body responds to PEDs at the lowest dosages of the mildest drugs and decide whether to continue using them.
Advantages
Because SARMs are not metabolized to dihydrotestosterone (DHT) by 5-alpha reductase, the risk of androgenic effect is reduced. This means that the risks to exposure to the prostate, acne, baldness are reduced, and the chances of excessive aggression caused by taking anabolic steroids are also reduced. In addition, SARMs are not metabolized by aromatase to estradiol, which limits estrogenic effects such as fluid retention, body fat gain, decreased libido and mood.
SARMs does not convert to estradiol, therefore they do not retain fluid in the body and do not have side effects associated with increased estradiol such as increased pressure due to fluid retention, mood swings, gynecomastia.
Basically, SARMs have less effect on suppressing HPTA and, accordingly, your own testosterone, if you do not exceed the average dosages. Keep in mind that in fact, only experimentally you will be able to determine which dosages are suitable for you personally, so that the suppression of testosterone would not be too great.
You will not experience many side effects (most likely there will be none) and such cycle will be very easy to administer, without the use of additional drugs such as aromatase inhibitors, cabergoline and others.
It is possible that your own testosterone will remain at normal levels, and you will not need PCT or it will be very minimal and your testosterone will quickly return to normal.
Disadvantages
As we described above, the advantage of SARMs is that they are not converted to estradiol and DHT, thus significantly reducing the side effects associated with these hormones. But as we know, these hormones also have their own positive effect on the body, so their indictors should always be in normal values. The growth of estradiol and DHT is always associated with a large amount of testosterone, which we introduce from the outside, because it is testosterone in this case that is their source (prohormone).
We also know that SARMs, although not as significant as steroids, still suppress the production of one’s own testosterone. As a result, after some time, when endogenous testosterone is suppressed, we are left only without testosterone, but also without normal levels of estradiol and DHT. Decreased levels of these hormones lead to decreased libido and mood, general fatigue and lack of energy/motivation. In addition, anabolism is also reduced, because both hormones are active anabolic agents. Low estradiol, these are problems with the lipid profile (cholesterol) and an increased risk of injuries to the articular- ligamentous apparatus, as well as a decrease in bone density. All this cannot be ignored and we must somehow increase the level of these hormones during the SARMs cycle.
For this reason, during the SARMs cycle, we resort to the use of drugs that will increase our testosterone levels, you will read about this further.
Long-term perspective
What I definitely see as an advantage is that if you are satisfied with the result you get- you can repeat this constantly for a long time, changing SARMs, dosages and duration- experimenting and studying your body’s reaction to all changes. Thus, within 4-5 years, you will get an impressive result and most importantly, you will not suffer from a drop in testosterone levels, as after regular cycles of anabolic steroids. Believe me- slowly and gradually, but surely and without hormonal pits- this is also a great option that can suit many. If I could turn back time, I would try this method.
Application scheme
Feel free to experiment with different dosages and cycle lengths, but start small – find your comfort zone between the most optimal dosages that give you the effect you want and the fewest side effects. The length of the cycle will always depend on your own goals, as well as on the results of blood tests. For example, if you do not want your testosterone to be completely suppressed during the cycle, you must carefully monitor its level with the help of tests. If it happens that despite the use of enclomiphene, your testosterone starts to fall below normal - this may serve as a signal to complete the cycle. Most often, PEDs users cycle from 8-16 weeks in which they try to achieve their goals – build muscle, increase strength or burn fat, but there is nothing to stop you from making your cycle shorter or longer. The advantage of SARMs in terms of cycle length over classic steroids is the significantly lower risk of side effects, due to which the cycle cannot be too long.
For whom it suits
To all those who are not in a hurry, want to look good, feel healthy, but do not chase competitive bodybuilding titles and do not have the desire to become a mass monster. With such a concept, I think your body over time can become very aesthetic, close to the body of athletes in the amateur nomination men’s physic. This is the body that most men want.
First of all, SARMs are suitable for those who have been training naturally for a long time and wants to take first steps towards applying some “boosters” to their results, but are not yet ready to use anabolic steroids. In this case, these drugs will be his first anabolics that will give a result, after which such an athlete will be able to decide whether he needs to try something more ‘heavy’ or not.
Perhaps, such a person will never want to get bigger or perform on a stage and will be able to create a form that suits him using only this type of drug, never touching anabolic steroids. There are plenty of people on Reddit who report that they have built fairly good muscle mass using only SARMs. This suggests that a new, safer generation of anabolic drugs may replace anabolic steroids altogether for many people.
What effect should expect
You should also understand that he result will be slightly lower in comparison with the classic cycle of steroids with testosterone. In total, it will most likely be 50% of the result that you would get from AS, but this is a security fee. Below we will present you a six-week cycle of SARMs and describe in detail what additional medications you will need to take so that you achieve maximum results and reduce all side effects, which, although unlikely, can still be.
SARMS and PCT
One of the biggest myths that resolves around the use of SARMs is that they do not effect the hormonal system, so PCT is not required. Any substance that activates the androgen receptor causes to a greater or lesser extent, a decrease in the endogenous production of sex hormones, primarily testosterone. Based on the real practice of athletes who used SARMs – even at the minimum dosages for muscle growth (20 mg Ostarine or 10 mg Ligandrol) – their own testosterone tends to zero after the 8th week of use. With these data in mind, we can safely say that after a SARMS cycle we almost need to use antiestrogen (SERMs) to bring our hormone levels back to normal.
Post Cycle Therapy (PCT) is the period immediately following the completion of a SARMS cycle when the user needs to return their hormone levels to normal with a combination of SERMs. It is important to note that since SARMs do not such a negative effect on the hypothalamic-pituitary -testicular arch as anabolic steroids, post-cycle therapy will not be as long and will most likely be easier with minimal dosages of clomiphene or tamoxifen.
After a SARM cycle, it is essential for users to replenish testosterone levels in their bodies. Without PCT, testosterone recovery will be slower and users may experience extreme fatigue and in some cases depression, as well as a drop in their scores. Taking PCT is important for maintaining overall well-being after the body has gone through a cycle of SARMs.
Usually, PCT after a SARMs cycle will look very simple – use Enclomilad 12.5-25 mg per day for some time until your testosterone reaches normal levels. You have to rely on blood tests to find out your testosterone level. Only these indicators can serve as a sign that PCT can be completed.
Testolone
Increases in muscle mass. RAD140 allows you to significantly increase muscle mass and give the body a more sculpted look and gives athletes a relief and powerful appearance and pronounced venousness. Athletes experience greater fullness and stiffness during the intake.
Also, according to reddit users, RAD140 significantly increases strength indicators and their growth is more pronounced even than a set of muscle mass. Great for strength and martial arts athletes. Decreased body fat and increased bone mineral density Suppresses own testosterone significantly compared to lighter compounds such as Ostarine and Andarine
HCG 5000
As we said earlier, due to the fact that SARMs will reduce your testosterone, you need to increase the level of this hormone with the help of other means that you will use throughout the cycle. Thus, you will stimulate the production of your own testsoteron, estradiol and DHT and avoid side effects that are associated with their low levels.
Gonadotropin, a drug that will be able to quickly and effectively increase your own testosterone and estradiol, and DHT, respectively through the stimulation of your testicles. The weekly dosage should be selected based on blood tests, which we recommend taking a week after the first injection, making adjustments if necessary.
The drug is used with small insulin syringes. You can use both intramuscular injections and subcutaneous injections, while using a fold on the abdomen. Injections made in this way are painless and very simple, so they should not frighten those who have not used injections before.
If you want to read about all the effects of this product - follow this link
https://driadashop.eu/hcg-5000iu-human-chorionic-gonadotropin?search=HCG
Enclomilad
One commonly used option is to use Enclomilad during SARMs cycle. Enclomilad will increase testosterone and thus estradiol and DHT levels. Enclomilad are taken daily. The dosage is usually the minimum required to maintain normal hormone levels.
If you want to read about all the effects of this product - follow this link
https://driadashop.eu/enclomilad-12-5-mg-enclomiphene-citrate
PEG-MGF
Mechanical growth factor (MGF) is a type of insulin-like growth factor (IGF-1), which is formed mainly after performing physical work, increases its secretion. Mechanical growth factor causes the division of myoblasts (germ muscle cells that are dormant), and also accelerates muscle growth and recovery. The effect is similar in many ways to growth hormone, but it does not strengthen bones and cartilage.
The physiological role of MGF has been highly studied in an in vitro cell model and in an experiment on mice. Unlike IGF-1, mechanical growth factor mainly causes the division of dormant muscle cells, due to the activation of various receptors. A decrease in the synthesis of MGF is the main reason, as a result of which there is a reduction in muscle mass in dystrophic patients and the elderly.
http://www.ncbi.nlm.nih.gov/pubmed/21354439
The average daily dose of Peg-MGF is 100-200 mcg, with a frequency of 2-3 times a week.
During the training days, the drug is administered immediately after training to simulate physiological secretion as much as possible, since the natural mechanical growth factor is released by the body in response to tissue damage.
Route of administration: subcutaneously with an insulin syringe.
The main effect that you can get from this peptide is muscle growth due to hyperplasia (acceleration of cell division), hypertrophy (increase in cell volume) which will have a positive effect on the regeneration of muscle tissue in case of injuries.
If you want to read about all the effects of this product - follow this link
https://driadashop.eu/peg-mgf-2mg
The drug is used with small insulin syringes. You can use both intramuscular injections and subcutaneous injections, while using a fold on the abdomen. Injections made in this way are painless and very simple, so they should not frighten those who have not used injections before.


